If you suffer from uterine fibroids—noncancerous tumors that grow on or in the muscle wall of the uterus—you may have heard of a fibroid treatment called uterine fibroid embolization, or ufe.
As ufe grows in popularity as a nonsurgical alternative to a hysterectomy, you might be wondering exactly what the procedure entails and what technology is used. Like with any medical procedure, understanding how it works in the body can help you and your doctor decide if this treatment is right for you.
What is ufe?
Uterine fibroid embolization is a minimally invasive procedure performed by an interventional radiologist. The doctor makes a small incision in the groin area and guides a catheter through the bloodstream to the fibroids.
There, small particles are inserted into the femoral artery to block the blood supply to the fibroids. Without an incoming supply of blood, the fibroids will stop growing and begin to shrink.
The procedure usually takes no more than an hour and you can often go home the same day, or after spending one night in the hospital. Recovery time is about 1-2 weeks, after which you can resume your normal day-to-day activities.
We found that 90% of women who have had this procedure report satisfaction at follow-up. Many notice an immediate improvement in their symptoms and in their own self-confidence.
What exactly are the particles used in ufe?
The particles that many interventional radiologists use are called Embosphere® Microspheres—gelatin beads similar to the consistency of soft contact lenses. The beads are very tiny, about the size of a poppy seed or grain of sand.
The size of the beads is carefully chosen by the interventional radiologist to ensure that only the blood supply to the fibroids is blocked and not the supply to the surrounding organs including the uterus.
The beads also have specific properties that help them do their job. These include non-aggregating properties, predictable distribution, and highly targeted delivery. Due to their texture and shape, the beads will not get stuck in the catheter or the artery, and therefore distribute as expected.
Embosphere Microspheres are the most clinically studied round embolic and have been used in procedures to help patients around the world.
Making the right choice for you
Uterine fibroid embolization is a safe, minimally invasive procedure for the treatment of uterine fibroids. It’s a viable option for many women who want to preserve their uterus and find relief from painful symptoms.
PLEASE NOTE: The above information should not be construed as providing specific medical advice, but rather to offer readers information to better understand their lives and health. It is not intended to provide an alternative to professional treatment or to replace the services of a physician.
Cheerful young Asian woman enjoying a tasty healthy bowl of yogurt at home
Eating more dairy may reduce your fibroid risk. If you’re a woman with uterine fibroids—a type of noncancerous growth found in the wall of the uterus—you may be familiar with this piece of advice.
Recent research suggests, however, that not necessarily all dairy is fibroid protective, but specifically yogurt—and the mineral calcium—are what may reduce fibroid risk.
With so many brands of yogurt to choose from, where do you begin? And what do you do if you’re lactose intolerant? Keep reading for dietitian-recommended tips and more to help guide you down the yogurt aisle.
When reading the ingredients, the list should be short: think milk, active cultures, and (depending on the brand) added vitamins.
Limit Sugar
High sugar intake can increase your risk of several chronic diseases. A recommended 10 grams of sugar or less per serving is what you should look for in a yogurt. Better yet, choose unsweetened brands and add Stevia and/or fresh fruit to sweeten your yogurt without added sugar.
Pay Attention to Fat Content
If you choose a non-fat yogurt, you can boost healthy fats by sprinkling toppings, such as nuts and seeds. If you like the taste and consistency fat brings to a yogurt, you can always opt for a 2 ̶ 4% milkfat content.
Don’t Forget Protein
When choosing a yogurt made from cow’s milk, look for brands that have at least 5 grams of protein per serving. Choosing a strained yogurt brand, such as Greek yogurt, can significantly increase your protein intake per serving.
Tips If You’re Lactose Intolerant
If you’re lactose intolerant, your body has a hard time digesting lactose—a type of sugar naturally found in dairy products. Eating or drinking dairy products (or foods made with dairy) can lead to uncomfortable symptoms, like stomach cramps, bloating, gas, diarrhea, and bouts of nausea.
If you’re lactose intolerant, below is a list of calcium-rich dairy alternatives to try.
Nut Milk
Nut milks, such as almond milk, macadamia milk, and pecan milk are healthy alternatives to cow’s milk because they’re fortified with calcium, often with a content much higher than dairy. Other plant milks, such as hemp seed milk, can be a great option, as it also contains omega-3 fatty acids, a natural anti-inflammatory agent.
Lactose-Free Milk
Although lactose-free milk is still cow’s milk, the lactose has been broken down to help your body digest it. In some brands of lactose-free milk, the lactose is filtered out altogether.
Plant Yogurts
Some dairy foods may be easier to digest for people with lactose intolerance, and yogurt is one of them. But for those who can’t digest dairy yogurt, plant yogurts are an exciting alternative to try. Made from coconut to flax seed to pea protein, these yogurts can be another healthful option.
Tips When Going Lactose-Free
Pass on Soy (for now)
Soy contains phytoestrogens, and it’s still unclear how soy impacts fibroid growth.
Avoid Added Sugars
Choose products that are low in sugar content (see above recommendation) or labeled “unsweetened.” As with dairy, try sweetening your yogurt with Stevia and/or fresh fruit.
Look for Calcium
The latest research suggests that it’s the calcium in foods that may be fibroid protective. Read the label to ensure your milk or yogurt has calcium, either naturally occurring or fortified.
Don’t give up!
Not all lactose-free foods will please your palate. Try different products to see which ones you like best.
For more on fibroids, treatment options, and other women’s health topics, read more on our blog.
Within the United States alone, about 26 million women between the ages of 15 and 50 have uterine fibroids. Of these women, 15 million are likely to have fibroid-related symptoms and health concerns, many needing treatment. Thankfully, a wide range of options exist—including minimally invasive approaches, like uterine fibroid embolization (ufe).
Unlike surgery, like hysterectomy or myomectomy, the ufe procedure requires nothing more than a small nick in the wrist of groin area. A doctor called an interventional radiologist inserts a slim tube called a catheter and guides it to the uterine arteries. Tiny particles called embolic are then delivered through the catheter to block the blood flowing to the fibroids. Once deprived of blood, fibroids begin to shrink, relieving symptoms, like heavy periods, pelvic pain, and urinary frequency.
A recent study published in the Journal of Personalized Medicine evaluated the clinical and radiological outcomes after ufe in 62 premenopausal women with symptomatic fibroids. All women underwent imaging of their fibroids (MRI or transvaginal ultrasound) before the procedure and then again at one-year follow up.
At follow-up, average fibroid diameter size was significantly reduced (42.6% ± 21.6%). There were also excellent improvements in both symptoms and quality of life, despite differences in fibroid size and number. No major complications were reported.
The researchers concluded, “The present study confirms the safety and efficacy of (ufe) in the treatment of symptomatic fibroids in pre-menopausal women with no desire to conceive.”
Two in three women will develop fibroids at some point in her life. Uterine fibroids are small, noncancerous growths that form on the wall of the uterus. Although benign, and while many women may not experience complications, for some, fibroid symptoms can be devastating. Worse, information on treatment options is not always made readily available, and many patients are led to believe that the only solution is major surgery—like a hysterectomy.
Meet Malin Florentzson, a woman who had her life turned upside down when doctors informed her that removing her uterus would be the best treatment for her heavy menstrual bleeding and pain.
“Being 28, I found it really shocking that they said it was absolutely the only option,” reflected Malin. “I decided not to do it and learn how to live with my problems.”
Malin gave it her all, but unfortunately, her symptoms caught up. When her pain and fatigue worsened to the point where she collapsed at an airport, she knew she needed to seek a second opinion. That’s when she discovered the source of her complications: fibroids.
As an employee of Merit Medical, Malin was familiar with uterine fibroid embolization (ufe). An alternative method of treating fibroids, ufe allows patients to preserve the uterus by stopping blood flow to the fibroids, which causes them to shrink—thus relieving symptoms.
For Malin, this presented an ideal solution. “I don’t want to remove an organ if I don’t absolutely have to,” she said. “I looked for someone to help me understand if I was a good candidate for ufe or not.”
After an Mri confirmed that ufe may be right for her condition, Malin scheduled an appointment with her gynecologist and interventional radiologist. And when the hospital placed the order with Merit for Embosphere® Microspheres—the tiny particles used to block blood supply to fibroids, causing them to shrink? It was Malin who took the call. “That was quite funny,” she remarked.
Malin made a full recovery from the successful ufe procedure. With her symptoms gone or significantly reduced, she was able to get back to the activities she enjoyed prior to developing fibroids. “It’s like a new life,” she said.
These days, Malin spends her time advocating for increased awareness of ufe as a treatment option to help reduce the stigma around talking about fibroids. “Who would I be if I couldn’t stand up and tell my story? We have to start understanding and listening to each other.”
Every woman’s body is different. There are all kinds of heights, shapes, hair colors, and shoe sizes. Menstrual cycles are no different. What seems normal for one woman could be completely out of the ordinary for another.
While some women have light periods and others are naturally heavier, there are times when heavy periods become extreme and can signal an underlying problem. So how do you tell the difference between normal and what is too much?
Should I be concerned?
A woman’s menstrual cycle can last anywhere from two to seven days and whether it’s heavy or light can depend on many factors. What’s normal is up to you and your body. However, if you suspect your period is heavier than it should be, there may be a problem.
Abnormally heavy bleeding is defined as being greater than 80 milliliters per cycle. Since this is often impossible to measure, a good way to tell is by judging the frequency at which you have to change your sanitary pad or tampon. If you have to change it every couple of hours or less, your bleeding may be heavier than normal.
Another way to judge is by the size and amount of blood clots in your period. If there is a lot of clotting or clots greater than one inch in diameter, this could also signal an underlying issue.
What causes heavy bleeding?
There are many factors that may be causing extreme bleeding. Often, it can simply be a hormone imbalance or change, such as the approach of menopause or the side effects of birth control.
Sometimes it can be a more serious problem. The following can all be causes of heavy menstrual bleeding:
Uterine cancer: This is a cancer that begins in the uterus and is usually characterized with abnormal bleeding, along with urinary pain or pain during intercourse.
Uterine fibroids: These are noncancerous tumors that grow on or in the muscular wall of the uterus. They often affect women in their 30’s and 40’s.
Infection: A main cause is pelvic inflammatory disease, which is an infection of a woman’s reproductive organs. It can cause serious damage if left unnoticed, but can be treated with antibiotics.
Extreme changes in weight: A restricted diet or high levels of stress can cause weight to fluctuate, which can trigger changes in the menstrual cycle.
Conditions related to pregnancy: A miscarriage can look like a heavy period. If you’re pregnant and you begin bleeding, call your doctor.
The best way to find out what is causing a heavy period is to talk to your doctor. Many problems like these can be detected early through something as simple as a physical exam or an ultrasound.
Treatment options
If your period is heavy due to a hormone change, it can often be reversed through hormone supplements or switching to a different type of contraceptive.
For some of the more severe issues, treatment can vary. Infections like pelvic inflammatory disorder can usually be treated with antibiotics. Cancer treatments depend on the stage and location of the cancer within the uterus, and can involve anything from chemotherapy to surgery.
For uterine fibroids, a procedure called uterine fibroid embolization maymake a world of difference. The treatment involves a small incision to the femoral artery and the injection of small spheres that block the blood flow to the fibroids, causing them to shrink.
No matter what the issue, make sure you talk to your doctor about what would be best for you. Just like every woman has a different shape, size, and menstrual cycle, treatment options vary for everyone. What works for one woman may not work for you.
PLEASE NOTE: The above information should not be construed as providing specific medical advice, but rather to offer readers information to better understand their lives and health. It is not intended to provide an alternative to professional treatment or to replace the services of a physician.
Humans have an innate relationship with the sun. Ancient civilizations worshipped it. Our 365-day calendar was created around it. And when bare skin is exposed to its ultra violet rays, the human body produces an essential nutrient—vitamin D.
Decades of studies have shown how vitamin D receptors are found in almost every cell of the body, influencing different levels of tissue and organ function. And now, emerging research is pinpointing how vitamin D, and more specifically sunlight exposure, may offer protection from chronic conditions like uterine fibroids.
Vitamin D, Sun Exposure, and Fibroids
A study published in Epidemiology evaluated 620 African American women and 416 Caucasian women, ages 35-49, in the National Institute of Environmental Health Sciences Uterine Fibroid Study.
Researchers determined participant vitamin D status by analyzing 25-hydroxy vitamin D levels (the precursor to active vitamin D) from collected blood samples. Ultrasound examinations were performed to establish the presence or absence of uterine fibroids. Additionally, data from a survey on self-reported sun exposure was gathered. Utilizing each piece of the puzzle, the authors then investigated whether vitamin D levels were associated with fibroid status in women.
Results of the study showed that women who had sufficient serum 25-hydroxy vitamin D levels, deemed as 20ng/mL or higher, had a 32% reduced risk of having fibroids when compared to those who had lower levels. Additionally, those who reported at least one hour per day of sun exposure also had a reduced risk.
Further investigation is needed, but these findings are consistent with results from previous in vitro studies and animal studies where treatment with active vitamin D metabolites slowed the growth of cultured uterine fibroid tissue. The authors concluded that “the consistency of [the current] findings provide evidence that sufficient vitamin D is associated with a reduced risk of uterine fibroids.”
How Much Sun Do I Need?
Exact recommendations are not easy to make. Individuals make vitamin D at different rates due to factors like skin pigment, age, season, and location in proximity to the equator. A person in Miami, Florida, for example, would need less time outside to receive the same sunshine benefits than someone in Boston, Massachusetts.
If you aren’t able to get enough sun or if you’re concerned about skin damage, a vitamin D supplement is another viable option. There are vitamin D food sources like fatty fish and egg yolks, but these foods probably won’t provide enough vitamin D.
The recommended daily allowance of vitamin D for adults 19-70 years of age is 600 IU. After 70, this amount increases to 800 IU. Although vitamin D shows promise and may naturally reduce the risk of fibroids, it’s still important to first discuss supplementation with your physician.
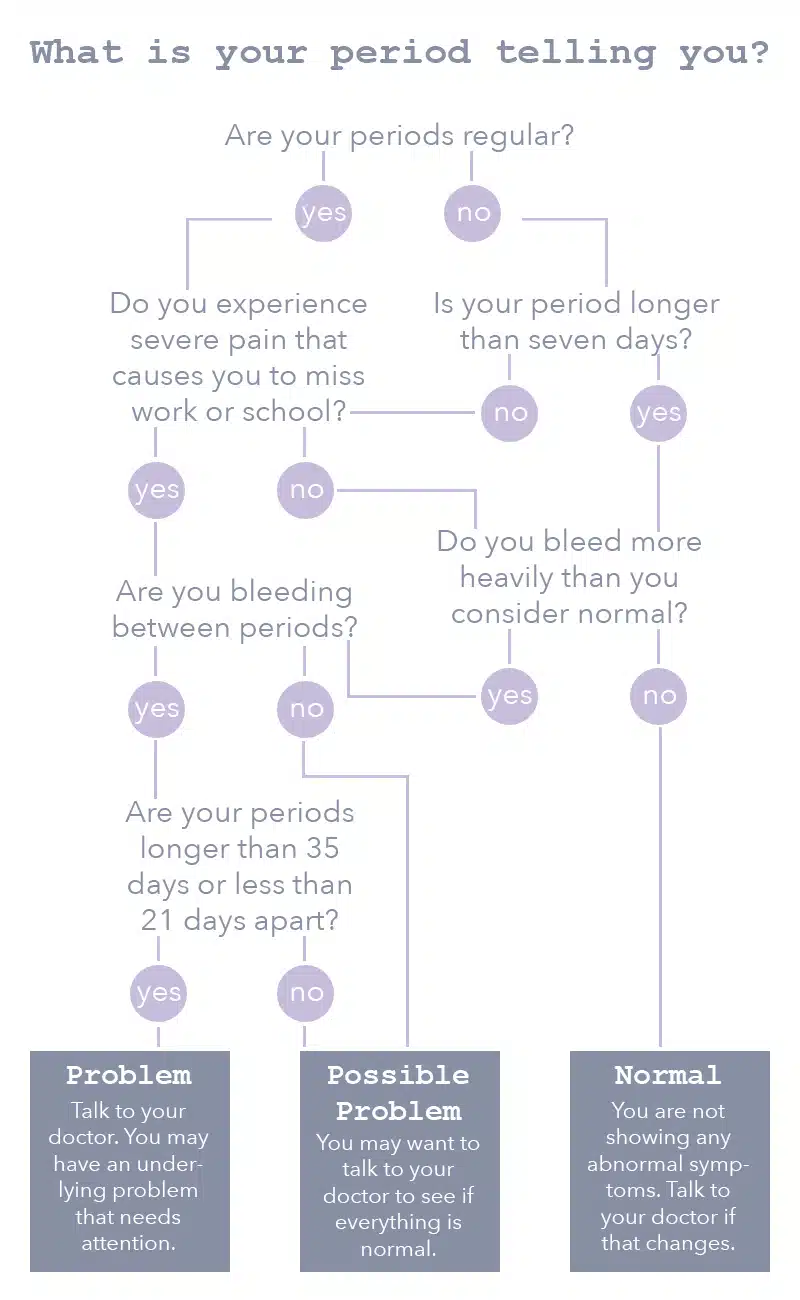
You may not think about it this way, but every month, your period is sending you signals. They may be signals that your body is healthy, and everything is as it should be—but the signals may also show that something is wrong.
Find out what your period may be telling you with this flowchart.
No matter what, everyone is different, so it’s important to have regular check-ups with your gynecologist to discuss your personal health history and find a care plan that’s right for you.
PLEASE NOTE: The above information should not be construed as providing specific medical advice but rather to offer readers information to better understand their lives and health. It is not intended to provide an alternative to professional treatment or to replace the services of a physician.
You’ve been diagnosed with uterine fibroids, and you’ve been given one option: hysterectomy. Thirty years ago, this scenario would be a common nightmare turned reality for women suffering with fibroid-related symptoms.
Fortunately, other minimally invasive treatment options have emerged. Uterine fibroid embolization (ufe) is one such option. Since introduced within the US in 1997 as a novel approach to treating fibroids, ufe has improved dramatically. From better tools to improved pain management, ufe continues to be a non-surgical, safe, and effective fibroid treatment option.
Unlike surgery, ufe requires nothing more than a small nick made in the wrist or groin area. A doctor called an interventional radiologist inserts a slim tube called a catheter and guides it to the uterine arteries. Tiny particles called embolic are then delivered through the catheter to block the blood flowing to the fibroids. Once deprived of blood, fibroids begin to shrink, relieving symptoms like heavy periods, pelvic pain, and urinary frequency for 90% of patients.1
Since its debut more than 20 years ago, ufe has continued to progress. Technological advancements of materials and tools used during the procedure have benefited both physicians and patients.
One area of ufe that has progressed by leaps and bounds has been that of the embolic material used. Initially, doctors only had two main choices: non-spherical polyvinyl alcohol (pva) particles and gelatin sponge. But these products seemed to come up short. Non-spherical PVA particles differed in size, making it difficult to use. Challenges like uncontrolled embolization during ufe and clogged catheters were common.2,3 The other option, gelatin sponge, was time consuming for doctors to prepare and trying to achieve same-size gel foam particles wasn’t easy.3
Given these setbacks, it was time for a next generation embolic. This led to the launch of Embosphere Microspheres, a spherical embolic that—to this day—is the most studied and clinically used embolic. It’s also considered the standard of care for ufe.4
What makes it different? Embosphere Microspheres particles are round and uniform in shape, giving doctors more control when treating women with ufe. Research has shown that all or nearly all (90% or more) of fibroid blood vessels are successfully blocked in 96% of ufe patients treated with Embosphere.5 This level of treatment is important because it has been shown to result in long-term clinical success and a lower rate of retreatment.6,7,8
Advances in imaging techniques have also made ufe an excellent approach to fibroid treatment. Ultrasound has generally been used to diagnose fibroids, but over time other imaging techniques have been proven to be more accurate. Magnetic resonance imaging (Mri), the current primary choice among interventional radiologists, provides information that ultrasound can’t. Studies have shown it to be better than ultrasound when it comes to observing uterine size, fibroid location, and number of fibroids.9,10 These pieces of information are important when determining if a woman is a good candidate for ufe and ruling out other causes of pelvic pain and bleeding.9
Managing pain during and after the procedure has also improved. “There have been several technical changes over the years to improve the ufe patient experience,” says Dr. Keith Pereira, assistant professor in the Division of Vascular & Interventional Radiology at Saint Louis University School of Medicine and a minimally invasive specialist at Saint Louis University Care Physician Group in Saint Louis, Mo., “During the procedure, we use a ‘flip of the wrist approach.’ This involves performing the entire procedure via a tiny pinhole in the artery in the wrist rather than the traditional approach through the groin. Patients are able to walk home with just a band-aid on their wrist.”
To counteract any discomfort felt after the procedure, Dr. Pereira describes applying a nerve block. “We use a temporary nerve block around the uterus for managing post-procedure pain. By numbing the nerves closest to the uterus, we’re able to offer patients pain-free ufe.”
Because of changes like these, Dr. Pereira explains that ufe has gone from being an inpatient procedure to an entirely outpatient procedure. “At our practice, no patient in the last year and a half has stayed more than three hours after a procedure. For example, a patient comes in skipping breakfast but goes home early enough to have lunch,” Dr. Pereira continues. “It has been a truly positive experience for our patients.”
Last but certainly not least, women can give themselves a pat on the back. By doing personal research, informing other women, and demanding better care, women have been a catalyst for change.
“Over the past ten years or so, we’ve had a renaissance of minimally invasive fibroid treatments, including ufe, that have made it possible for women to find relief without surgery,” says Dr. Todd Harris, surgeon and fibroid specialist at The Fibroid Treatment Center in Newport Beach, Calif., and founder of The Fibroid Treatment Network. “Online education has revolutionized the ability for women to find doctors who provide the entire spectrum of care or who are willing to refer out to other doctors to make sure they get the treatment they need.”
This progress demonstrates significant steps forward in fibroid care and women’s health. We’re looking forward to even more improvements being made in the years to come.
ABOUT THE DOCTORS
Keith Pereira, MD, is assistant professor in the Department of Radiology, Division of Vascular & Interventional Radiology, at Saint Louis University School of Medicine and a minimally invasive specialist at Saint Louis University Care Physician Group. Besides being among the first to perform ufe via the radial artery in the wrist and combining this with the uterine nerve block, he uses minimally invasive, non-surgical procedures to treat conditions like blocked arteries and veins in the legs, prostate enlargement in men, and liver and kidney cancer.
Todd S. Harris, MD, is medical director of The Fibroid Treatment Center. Board certified in general surgery, as well as fellowship trained in interventional radiology, Dr. Harris is highly experienced in fibroid surgery. Dr. Harris shares his knowledge and expertise by actively engaging in research and participating in volunteer work around the globe.
REFERENCES
Silberzweig, J. E., Powell, D. K., Matsumoto, A. H., et al. (2016). Management of uterine fibroids: a focus on uterine-sparing interventional techniques. Radiology, Sep;280(3):675-692.
Pelage, J., Laurent, A., Wassef, M., et al. (2002). Uterine artery embolization in sheep: Comparison of acute effects with polyvinyl alcohol particles and calibrated microspheres. Radiology, Aug;224(2):436-445.
Worthington–Kirsch, R. (2008, Jun). Do Particle Size and Type Matter? Endovascular Today.
Duvnjak, S., Ravn, P., Green, A., et al. (2017). Assessment of uterine fibroid infarction after embolization with tris-acryl gelatin microspheres. Cogent Med, Aug;4(1):1360543.
Katsumori, T., Kasahara, T., Kin, Y., et al. (2008). Infarction of uterine fibroids after embolization: Relationship between postprocedural enhanced Mri findings and long-term clinical outcomes. Cardiovasc Intervent Radiol, Jan-Feb;31(1):66–72.
Koesters, C., Powerski, M. J., Froeling, V., et al. (2012). Uterine artery embolization in single symptomatic leiomyoma: Do anatomical imaging criteria predict clinical presentation and long-term outcome? Acta Radiol, May;55(4):441–449.
Kroencke, T. J., Scheurig, C., Poellinger, A., et al. (2010). Uterine artery embolization for leiomyomas: Percentage of infarction predicts clinical outcome. Radiology, Jun;255(3):834–841.
Gonsalves, C. (2008). Uterine artery embolization for treatment of symptomatic fibroids. Semin Intervent Radiol, Dec;25(4):369-377.
Spielmann, A. L., Keogh, C., Forster, B. B., et al. (2006). Comparison of Mri and sonography in the preliminary evaluation for fibroid embolization. AJR Am J Roentgenol, Dec;187(6):1499-504.
For more information please refer to Instructions for Use. Consult product labels for any indications, contraindications, potential complications, warnings, precautions and directions for use. Dr. Siskin is a paid consultant of Merit Medical Systems, Inc.
Being diagnosed with uterine fibroids may be overwhelming. But fortunately, you have options—and lots of them. From pharmaceutical treatments to surgery, and less-invasive options in between, a woman has much to choose from.
NON-INVASIVE TREATMENT OPTIONS
Pharmaceutical Treatment
Non-steroidal anti-inflammatory drugs (Nsaids), like ibuprofen, can reduce menstrual flow by 25-30 percent and lessen cramping.1 Hormonal birth control options2,3 like the pill, patch, vaginal ring, injections, and intrauterine devices have also been found to reduce bleeding—but not fibroid size. Iron supplementation1 may be needed to combat anemia that can result from heavy periods. Although some of these options are available over-the-counter, use and duration of therapy should be discussed with your doctor first.
GnRh-a Therapy
GnRH-a, or Gonadotropin-releasing hormone analogue therapy, may be used to shrink fibroids and reduce menstrual bleeding. Fibroid symptoms may cease when starting therapy but will return once treatment stops.
GnRH-a therapy preserves the uterus but has been linked to causing menopausal-like symptoms, such as hot flashes, decreased sex drive, spotting, fatigue, depression, and bone loss.4 For this reason, it’s commonly used as a short-term option to shrink fibroids before their surgical removal.2
MR-Guided Focused Ultrasound (MrgFus)
Also known as high intensity focused ultrasound or HIFU, this procedure uses ultrasound waves to penetrate the abdominal wall and heat fibroid tissue causing it to shrink by up to 54 percent one year after the procedure, according to research.5
This uterus and fertility-sparing option can take several hours to complete but is associated with less than one week of recovery time and minimal discomfort.
The success of MRgFUS depends on fibroid location since it’s most effective at treating small fibroids located near the uterine surface. A risk of fibroid recurrence exists and more than one procedure may be needed.
LESS-INVASIVE TREATMENTS
Uterine Fibroid Embolization (ufe)
Performed by an interventional radiologist, ufe is a minimally-invasive, non-surgical option that shrinks fibroids.
The physician makes a small incision in the upper thigh or wrist to access the arteries providing blood to the fibroids. Tiny spheres called embolics are injected into the arteries, blocking the blood flow, causing the fibroids to shrink and die. After the procedure, cramping and flu-like symptoms may occur, but can be treated and typically subside after 12 hours.6 Women can return to normal activity, on average, within 11 days. ufe has a 90 percent cure rate of symptoms7 and is effective treating fibroids of all sizes, but risk of recurrence does exist, in some cases warranting further rounds of treatment.
Endometrial Ablation
Endometrial ablation destroys the lining of the uterus with the goal of reducing heavy menstrual bleeding. By inserting tools into the uterus through the vagina, ablation methods include radiofrequency, freezing, heated fluid, microwave energy, and electrosurgery.8 Since the lining is targeted, this option effectively treats submucosal fibroids that measure less than one inch in diameter. Since endometrial ablation doesn’t reduce fibroid size, it doesn’t treat symptoms related to fibroid bulk such as pain, pressure, or urinary incontinence.
Abnormal bleeding can recur and additional procedures may be needed. Although uterus-sparing, women who wish to become pregnant should avoid this procedure.
Radiofrequency Ablation
Performed laparoscopically and as an outpatient procedure, radiofrequency ablation works by inserting a needle-probe into the middle of each fibroid. Heat is delivered through the probe, destroying and shrinking fibroid tissue.
Recovery time is minimal with women reportedly returning to work in less than a week. The procedure may take several hours and there’s a risk of fibroid recurrence. However, studies indicate a high rate of patient satisfaction, significant reductions in symptom severity, and an increase in quality of life.9
SURGICAL TREATMENTS
Myomectomy
Myomectomy, or the surgical removal of fibroids, has been considered the go-to treatment for women wanting to alleviate symptoms while still maintaining their fertility. Surgical methods include hysteroscopic, laparoscopic (including robotic), and abdominal. Risks include those associated with surgery, including extensive blood loss and scar tissue. Recovery time can last up to six weeks and fibroids may recur, requiring more surgery over time.
Hysterectomy
A hysterectomy surgically removes the entire uterus and is an option for women who no longer wish to conceive. Doing so leads to permanent symptom relief but other side effects such as pelvic and back pain, sexual dysfunction, and incontinence. Side effects may intensify with ovary removal.
As seen with myomectomy, additional risks include those linked with surgery and general anesthesia. Different types of hysterectomy are available and differ depending on whether other structures surrounding the uterus are also removed. Recovery time averages between two and six weeks.
And what if you don’t have symptoms? The best option may be to simply monitor your fibroids under the supervision of your doctor.
In the end, the best decision a woman can make regarding her fibroid treatment is one she’s made with confidence and a well-informed mind.
2. Khan, A. T., Shehmar, M., & Gupta, J. (2014). Uterine fibroids: current perspectives. International Journal of Women’s Health, 6: 95-114. doi: 10.2147/IJWH.S51083
3. Zapata, L. B., Whiteman, M. K., Tepper, N. K., Jamieson, D. J., Marchbanks, P. A., & Curtis, K. M. (2010). Intrauterine device use among women with uterine fibroids: a systematic review. Contraception, 82(1): 41-55. doi: 10.1016/j.Contraception.2010.02.011
4. Magon, N. (2011). Gonadotropin releasing hormone agonists: expanding vistas. Indian Journal of Endocrinology ad Metabolism, 15(4): 261-267. doi: 10.4103/2230-8210.85575
5. Bohlmann, M. K., Hoellen, F., Hunold, P., & David, M. (2014). High-intensity focused ultrasound ablation of uterine fibroids-potential impact on fertility and pregnancy outcome. Geburtshilfe Frauenheilkd, 74(2): 139-145.doi: 10.1055/s-0033-1360311
6. Spencer, E. B., Stratil, P., & Mizones, H. (2013). Clinical and periprocedural pain management for uterine artery embolization. Seminars in Interventional Radiology, 30(4): 354-363. doi: 10.1055/s-0033-1359729
7. McLucas, B., Voorhees Iii, W. D., & Elliott, S. (2015). Fertility after uterine artery embolization: a review. Minimally Invasive Therapy & Allied Technologies, 2: 1-7.
9. Chudnoff, S. G., Berman, J. M., Levine, D. J., Harris, M., Guido, R. S., & Banks, E. (2013). Outpatient procedure for the treatment and relief of symptomatic uterine myomas. Obstetrics & Gynecology, 121(5): 1075-1082. doi: 10.1097/AOG.0b013e31828b796
As you’re considering how to treat your uterine fibroids, you probably want to know the details of all the different options: how to prepare, what to expect during the procedure, and how recovery will be.
With uterine fibroid embolization (ufe), it’s no different. You know the pros and cons, but you want to learn more, and the best place to find the answers is with the interventional radiologist who will be performing the procedure. Use these five questions to get the conversation started.
1. How often is the procedure successful?
The particles used in ufe are inserted into the uterine artery, which supplies 99% of blood flow to the fibroids. When this blood supply is blocked, all of the fibroids are treated, meaning that the procedure will be successful.
Occasionally, the fibroid is getting enough blood from another source to stay alive. Normally, this will be identified and treated at the same time as the uterine artery, but if it is not identified, another procedure may be required.
However, as one doctor reported, the success rate is about 95-98% for good candidates of the procedure.
2. Are your patients happy with ufe?
The statistics show that around 90% of patients are satisfied at follow-up. Dr. Linda Hughes, an interventional radiologist in Miami, FL, puts it this way:
“Yes, typically patients are very happy with the procedure in terms of the short amount of time it take for the procedure itself, the short recovery time and how quickly they see results from the procedure.”
3. What are typical complications and how often do they occur?
With ufe, complications are very rare. As with any surgical procedure, infection is possible, but it happens with very few patients.
Other than infection, there is the risk of ovarian failure or premature menopause, which affect less than 2% of patients. If that were to occur, the patient would work with her gynecologist to begin hormone replacement if possible.
4. How long should I expect to be in recovery?
After the procedure, you will likely stay in the hospital for one night so the nurses and doctors can continue to monitor how you’re doing. You will experience moderate cramping in the pelvis for up to 6 hours after the procedure is performed.
Once you return home, you may be affected by “post-embolization syndrome,” which has been described by previous patients as flu-like symptoms – fatigue, fever, nausea, and achiness. This usually goes away in 3-5 days.
Most patients are able to return to work and light activities within 7-14 days, which differs from person to person. More strenuous activity should not be attempted until at least two weeks after the treatment.
5. Will my fibroids or symptoms come back?
Since UFE blocks the blood supply to all the fibroids, there is a very low chance that they will come back. If there is another source supplying the fibroids with blood, there is a possibility that they could continue to grow, but if so, that supply can be treated.
UFE shrinks the fibroids to 40-60% of their original size, so while they will likely remain, you will not experience any more painful and frustrating symptoms.
Learn more
Your conversation with your doctor shouldn’t stop here. To hear interventional radiologists’ answers to these questions and more, visit our Videos page.
PLEASE NOTE: The above information should not be construed as providing specific medical advice, but rather to offer readers information to better understand their lives and health. It is not intended to provide an alternative to professional treatment or to replace the services of a physician.
We may request cookies to be set on your device. We use cookies to let us know when you visit our websites, how you interact with us, to enrich your user experience, and to customize your relationship with our website.
Click on the different category headings to find out more. You can also change some of your preferences. Note that blocking some types of cookies may impact your experience on our websites and the services we are able to offer.
Essential Website Cookies
These cookies are strictly necessary to provide you with services available through our website and to use some of its features.
Because these cookies are strictly necessary to deliver the website, refusing them will have impact how our site functions. You always can block or delete cookies by changing your browser settings and force blocking all cookies on this website. But this will always prompt you to accept/refuse cookies when revisiting our site.
We fully respect if you want to refuse cookies but to avoid asking you again and again kindly allow us to store a cookie for that. You are free to opt out any time or opt in for other cookies to get a better experience. If you refuse cookies we will remove all set cookies in our domain.
We provide you with a list of stored cookies on your computer in our domain so you can check what we stored. Due to security reasons we are not able to show or modify cookies from other domains. You can check these in your browser security settings.
Other external services
We also use different external services like Google Webfonts, Google Maps, and external Video providers. Since these providers may collect personal data like your IP address we allow you to block them here. Please be aware that this might heavily reduce the functionality and appearance of our site. Changes will take effect once you reload the page.